



Hide
Los hombres sometidos a prostatectomías laparoscópicas vuelven a gozar de una función urinaria completamente normal y voluntaria, sin incomodidades o signos de obstrucción, pasados unos tres meses después de la cirugía.
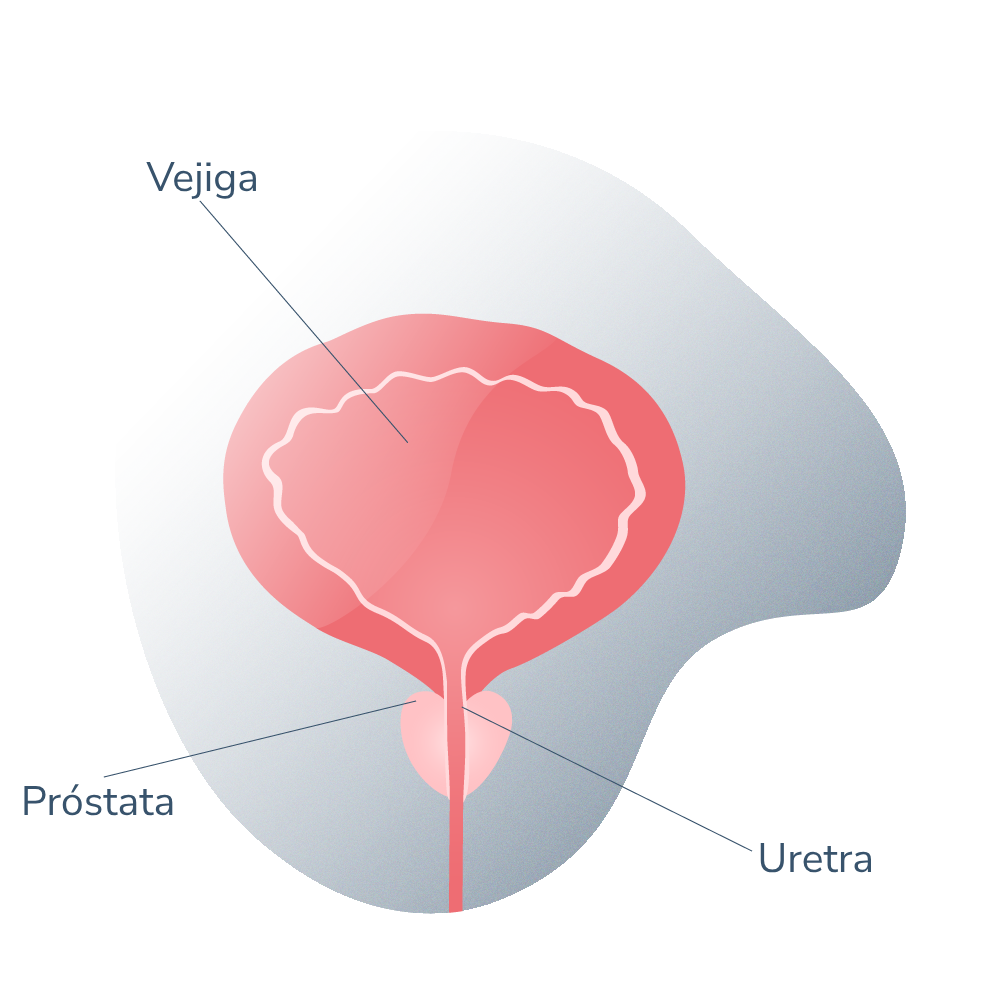
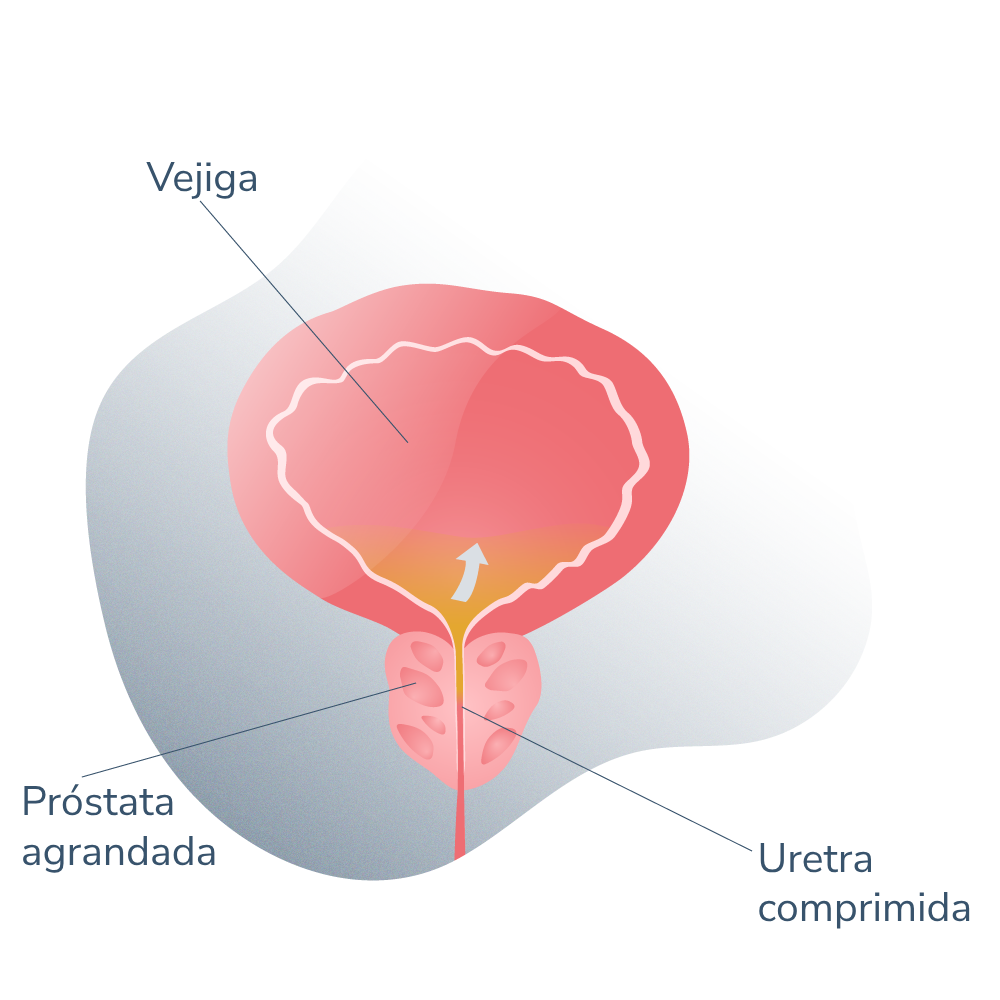
Hay que tener en cuenta el importante porcentaje de pacientes que, a causa de los trastornos prostáticos (como la hiperplasia benigna de próstata o los tumores malignos de la glándula) perdieron la capacidad de orinar con tranquilidad, así que tres meses es un tiempo más que positivo para recuperar esta función.
Después de la cirugía, el médico dará indicaciones específicas sobre el cuidado del sitio de la operación para acelerar el proceso de recuperación y cicatrización. Más específicamente, de las incisiones que fueron realizadas en la piel y, para ello, los cuidados son los siguientes:
• Colocar adhesivo estéril, especial para estos casos, en el sitio de las incisiones durante unos 10 días a dos semanas después de la intervención. Esto ayudará a que cada incisión permanezca lo más seca, limpia y protegida posible del roce de la ropa.
• Evitar tomar aspirina para tratar el dolor, en ese caso, es posible tomar analgésicos sin receta como el acetaminofén.
• Es normal que la piel cercana a los sitios de incisión cambie de color y se torne un poco azulada u oscura. Esto es completamente normal y desaparecerá por sí solo al cabo de un par de días.
• Cuándo volver a conducir un coche es una pregunta frecuente entre los hombres sometidos a esta cirugía y la verdad es que no existe un tiempo establecido, pero en la mayoría de los pacientes pueden volver a hacerlo en unos 10 a 14 días. Todo esto depende de las indicaciones del médico.
 La disfunción eréctil (DE) representa el riesgo más importante y con mayor prevalencia que se corre al realizar una prostatectomía radical, sea cual fuere su modalidad quirúrgica.
Evidentemente, los médicos guardan mucho cuidado al realizar la extirpación de la próstata y de dejar intactos el conjunto de nervios que inervan al pene y las estructuras genitales. Sin embargo, la anatomía indica que existe una estrecha relación entre la glándula y estos nervios, por lo que al extraerlo también se lleva consigo algo de nervios, disminuyendo la sensibilidad de la zona y la respuesta eréctil de los cuerpos cavernosos.
No obstante, no todo está perdido. Si ocurre impotencia sexual masculina, disfunción eréctil o erecciones débiles pueden recurrirse a otros métodos terapéuticos para mantener la vida sexual activa de los pacientes. Estos métodos terapéuticos incluyen:
La disfunción eréctil (DE) representa el riesgo más importante y con mayor prevalencia que se corre al realizar una prostatectomía radical, sea cual fuere su modalidad quirúrgica.
Evidentemente, los médicos guardan mucho cuidado al realizar la extirpación de la próstata y de dejar intactos el conjunto de nervios que inervan al pene y las estructuras genitales. Sin embargo, la anatomía indica que existe una estrecha relación entre la glándula y estos nervios, por lo que al extraerlo también se lleva consigo algo de nervios, disminuyendo la sensibilidad de la zona y la respuesta eréctil de los cuerpos cavernosos.
No obstante, no todo está perdido. Si ocurre impotencia sexual masculina, disfunción eréctil o erecciones débiles pueden recurrirse a otros métodos terapéuticos para mantener la vida sexual activa de los pacientes. Estos métodos terapéuticos incluyen:
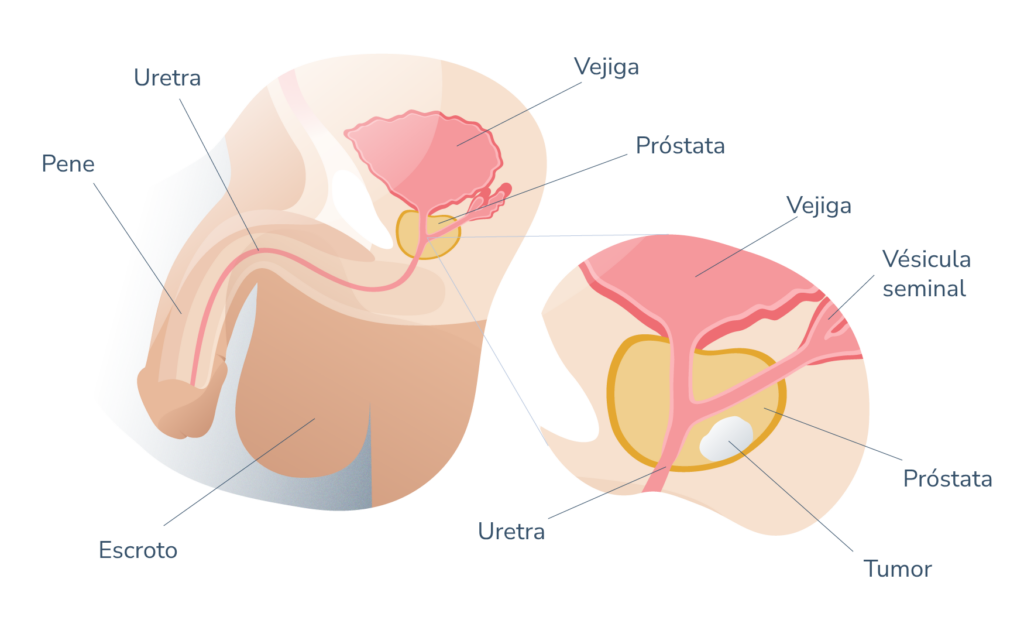
No, debido a que la próstata que será eventualmente extraída no tiene como función la producción de espermatozoides (esto ocurre en los testículos, dentro del escroto).
Después de la cirugía, las eyaculaciones serán un poco menos abundantes (porque la próstata produce parte del semen) pero la capacidad de fertilizar sigue intacta a menos que haya problemas en los testículos.
Si te encuentras en el periodo de recuperación y notas los siguientes síntomas es importante llamar al médico o acudir a consulta:
• Fiebre mayor de 40° C.
• Si el dolor es muy fuerte o no desaparece con los analgésicos indicados.
• Dificultad para orinar o sangre en la orina.
• Mareos y vértigo.
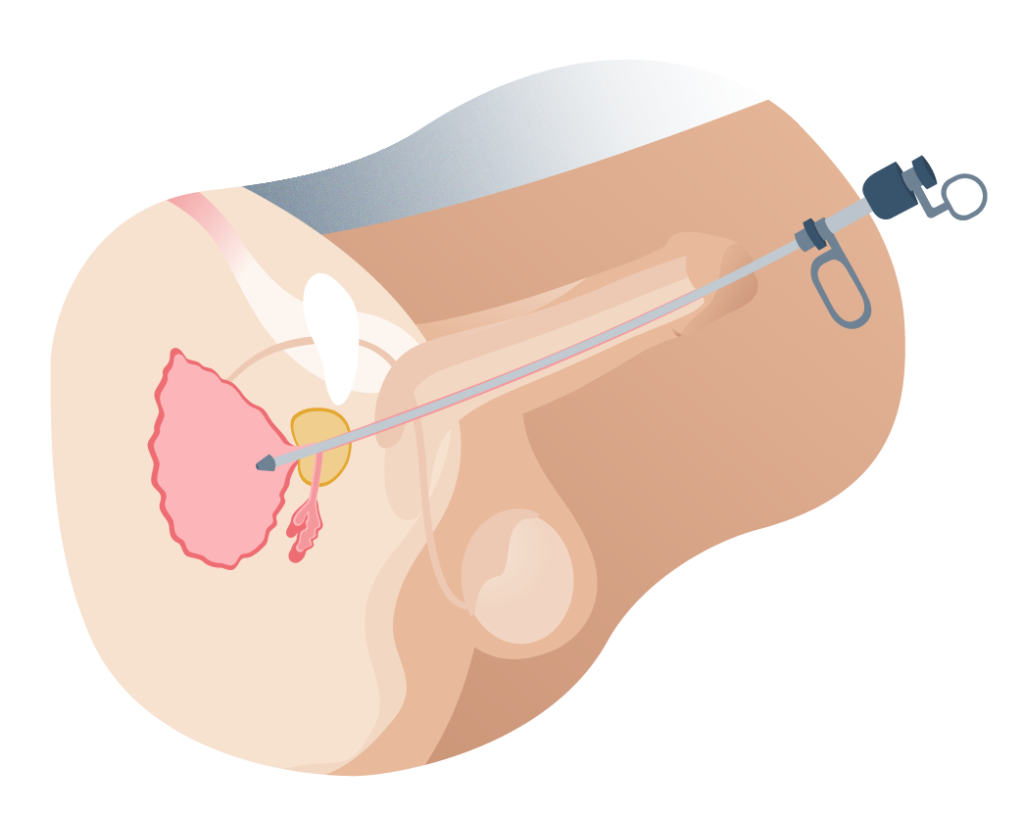
Sí, es necesario usar catéter o sonda vesical durante algún tiempo posterior a la cirugía de prostatectomía radical debido a que se requiere dar oportunidad a los tejidos uretrales a que se reconecten y cicatricen. Generalmente se requieren entre dos y tres semanas con sonda.
Todo paciente masculino con diagnóstico de cáncer de próstata localizado sin metástasis puede ser candidato a la prostatectomía radical laparoscópica.
No obstante, cada caso debe ser atendido y valorado de manera individual puesto que en contados casos, un tumor no tan bien localizado dentro del tejido glandular prostático puede ser abordado por métodos laparoscópicos.
Los médicos recomiendan abstinencia sexual absoluta durante un mes después de una intervención de este tipo. Esta abstinencia incluye relaciones sexuales con penetración, masturbación y eyaculación (la eyaculación podría ser dolorosa o con algo de sangre).
Desarrollar problemas eréctiles menores después de haber sido eliminado un órgano potencialmente peligroso para la vida del paciente es algo menor. De hecho, es algo infrecuente con esta técnica y los hombres siguen gozando de una vida sexual activa y plena.
En muchos otros casos, la disfunción eréctil ya era un problema de base. Es decir, ya estaba presente antes de la cirugía (especialmente en pacientes obesos, diabéticos, hipertensos o de edad muy avanzada).
Dentro de las alternativas para tratar la disfunción eréctil se encuentran:
• Medicamentos inhibidores de la fosfodiesterasa 5 como el sildenafilo, el taladafilo o el vardenafilo que favorecen la relajación de los vasos sanguíneos que van al pene y por ende, los mecanismos de la erección se potencian.
• Inyecciones intracavernosas de alprostadil, un medicamento con efecto vasodilatador que se infiltra en la base de los cuerpos cavernosos del pene y tiene un efecto prolongado.
• Bombas de vacío, unos dispositivos de succión en los que se inserta el pene en estado de flacidez para inducir la erección.
• Cirugía de implantes peneanos, una solución definitiva y quirúrgica al problema.

Laparoscopic surgery for prostate
26 September 2023


Laser prostate surgery
22 November 2021


Impotence, incontinence and other problems after prostate surgery
22 November 2021