Técnica de Shaeer para curvatura congénita del pene
Miles de hombres alrededor del mundo padecen hoy serios problemas para conseguir erecciones firmes y sin dolor, ellos padecen de curvatura congénita del pene. Un trastorno de los cuerpos cavernosos, de una deformidad pero que tiene solución y en este artículo intentaremos abordarlos, especialmente la técnica de Shaeer o de rotación de cuerpos, una de las más eficaces.
- VÍDEO: Tratamientos y técnicas para corregir la curvatura de pene, pene curvo o pene torcido
¿Qué es la curvatura congénita del pene?
La curvatura congénita del pene (o CPC) es causada por un desarrollo embrionario anormal en el cual los cuerpos cavernosos crecen asimétricamente, produciendo una incurvación del órgano que se hace pronunciada durante la erección.
Esta curvatura peneana durante la erección en los hombres afectados, generalmente es ventral (o hacia adelante) y puede llegar ser tan severa (incluso más de 90 grados) que las relaciones sexuales pueden ser muy difíciles o incluso imposibles.
La curvatura de pene es una condición bastante común en la oficina de Andrología. Puede afectar seriamente las relaciones sexuales y puede ser la causa de mayor preocupación psicológica. Se requerirá un cuidado especial por parte del especialista y un enfoque sensible.
Una asimetría o desproporción entre los dos cuerpos cavernosos o entre los cuerpos cavernosos y el cuerpo esponjoso, puede causar una curva congénita del pene. Los cuerpos cavernosos normales son simétricos y elásticos, lo que permite que el pene mantenga una posición recta durante la erección. Sin embargo, la curvatura congénita del pene es causada por el acortamiento que afecta, con mayor frecuencia, la parte ventral del pene.
Por lo general, el agujero uretral (por donde sale la orina) tiene una ubicación normal en la punta del glande pero el prepucio puede estar incompleto mostrando una forma de capuchón dorsal y el rafe anterior (o frenillo) presenta fibrosis y muestra signos de tensión. En casos severos, la uretra puede presentar problemas para transportar la orina hacia el exterior.
Looking for prices and information?
Use our virtual assistant and receive in your email everything related to the treatments that interest you. Budgets, recovery times, hospitalization, financing possibilities month by month, etc.
In just a few minutes and without any commitment.
En cumplimiento del Reglamento General de Protección de Datos le informamos que los datos por Vd. proporcionados serán objeto de tratamiento por parte de Andromedi con la finalidad de prestarle el servicio solicitado y/o contratado. Los datos no se cederán a terceros salvo en los casos en que exista una obligación legal. Para más información puede consultarla pinchando aquí.
Tipos de curvatura congénita de pene
Se pueden encontrar dos tipos principales de curvatura congénita del pene que dependerán del desarrollo del cuerpo esponjoso (por donde pasa la uretra con la orina), la primera está asociada con una uretra normal y la segunda con aquellos con uretra hipoplásica o más corta de lo normal. Esto último puede traer serios problemas para orinar.
Desde el año 1991, existe una clasificación para agrupar los distintos tipos de curvatura congénita de pene de acuerdo a las estructuras afectadas por el defecto anatómico del desarrollo embrionario:
- Tipo I: afecta el esponjoso, los dartos y la fascia de Buck. El meato uretral tiene una posición normal en el glande pero hay una falta total de desarrollo de todas las capas que rodean la uretra. La uretra, sin cuerpo esponjoso, está muy adherida a la piel y por eso la retrae, causando la deformidad.
- Tipo II: afecta la fascia de Buck y Dartos. La uretra está rodeada por un cuerpo esponjoso normal pero el tejido mesenquimatoso (del cual se originó la fascia y los dartos de Buck) desarrolla dos bandas de tejido fibroso que se extienden profunda y lateralmente a lo largo del tejido esponjoso. Produciendo una retracción del tejido.
- Tipo III: afecta la fascia de los Dartos, presentando una adhesión anormal de la fascia de Buck y el cuerpo esponjoso a la piel del prepucio.
- Tipo IV: afecta la albugínea de los cuerpos cavernosos. La uretra y las fascias circundantes se desarrollan normalmente, pero hay un acortamiento y desarrollo inelástico de la túnica albugínea de los cuerpos cavernosos
- Tipo V: solo afecta el cuerpo esponjoso pero causando un acortamiento uretral bastante grave
De todos estos tipos, la presentación más severa es el tipo I. Una condición en la cual el esponjoso es más corto de lo normal y la curvatura del pene ventral está en gran medida condicionada por la falta de desarrollo de la uretra y la desproporción que existe entre el cuerpo esponjoso y el cavernoso.
Es probable que dentro de la terminología utilizada en la literatura médica para esta afección probablemente debería revisarse que los términos “curvatura congénita del pene” y “cuerda sin hipospadias” a menudo se han usado indistintamente.
El término cuerda sin hipospadias se usa para aquellos pacientes en los que el meato o agujero urinario está ubicado adecuadamente en la punta del glande y una curvatura ventral está claramente asociada con anomalías congénitas del cuerpo esponjoso, los tejidos de las fascias ventrales o ambos. En una revisión reciente, Makovev et al. definió la curvatura congénita del pene como resultado del desarrollo desproporcionado de la túnica albugínea de los cuerpos corporales cavernosos, que no está asociada con la malformación uretral.
Se necesita un enfoque diferente para estos dos tipos principales de curvatura congénita. La conciencia sobre el posible acortamiento uretral o la falta congénita de estas estructuras es el problema clínico más relevante en este punto.
Tipos de curvatura congénita de pene
La curvatura congénita del pene es la segunda causa más común de curvatura del pene después de la enfermedad de La Peyronie. La prevalencia publicada parece indicar una condición frecuente, que afecta al 4% -10% de los hombres. Autores como Ebbehoj y Metz investigaron su incidencia en la población danesa e informaron una incidencia de 0,37 por cada mil nacimientos masculinos. Otros investigadores como Yachia y col. informó una incidencia de menos del 1%.
No obstante, muchos otros investigadores creen que el CPC tiene una mayor incidencia y prevalencia que lo informado. La presencia de CPC en la infancia es difícil de identificar y su prevalencia real en adultos también es difícil de evaluar. Incluso hoy, el CPC se acepta como normal o se considera irreparable. Muchos hombres viven con su anormalidad peneana en una soledad absoluta y abrumadora.
¿Por qué se produce la curvatura congénita del pene?
No existe aún una evidencia de la causa real de la curvatura congénita del pene. Sin embargo, se han sugerido varios mecanismos como los siguientes:
- Un defecto embriológico del desarrollo normal del pene (dentro del útero materno), por una desregulación de la testosterona que se convierte por 5-alfa-reductasa en dihidrotestosterona (DHT), la sustancia encargada de inducir un apropiado desarrollo de los genitales masculinos.
- Deficiencia de andrógenos o insensibilidad a los mismos.
- Un estudio único que analiza la ultraestructura de la túnica albugínea ha demostrado ensanchamiento y fragmentación de las fibras de colágeno, con ausencia total de estriación y transformación en material granulado fibroso denso en electrones y acumulación de elastina. El colágeno es necesario para la consistencia de las células de los cuerpos cavernosos.
Presentación clínica y evaluación del paciente
Los pacientes que sufren de curvatura congénita de pene generalmente asisten a la oficina de los médicos cuando se vuelven sexualmente activos, es decir, en la segunda o tercera década de la vida. Solo los casos más graves de cordón sin hipospadias pueden diagnosticarse en la infancia debido a los problemas que tienen para orinar. Estos pacientes generalmente se quejan de curvatura del pene erecto; que a menudo es ventral o hacia adelante, a veces lateral y raramente dorsal o hacia atrás. En algunos casos, el pene puede incurvarse hacia dos direcciones (como ventral y lateral, al mismo tiempo). La curvatura dorsal es extremadamente rara excepto cuando está asociada con la torsión del pene.
Una curvatura mínima de menos de 15 ° es común y clínicamente no relevante, siempre que las erecciones sean indoloras y no interfieran con las relaciones sexuales. Cuando la curvatura es mayor de 30 ° el paciente puede tener dificultades con las relaciones sexuales o molestias por penetración, además de las preocupaciones estéticas. La función eréctil es normal, pero puede verse comprometida por una curvatura excesiva.
¿Cómo se realiza un correcto diagnóstico?
Los historiales médicos y sexuales suelen ser suficientes para establecer el diagnóstico de curvatura congénita del pene. Esto se logra con una adecuada entrevista médica que permita obtener información relevante sobre el estado general de salud del paciente, los antecedentes familiares y los hábitos sexuales y de vida que desempeña.
El examen físico, durante la erección, es útil al documentar la curvatura y excluir otras patologías como la enfermedad de La Peyronie que suele ser algo más complicada.
Se recomiendan autofotografías del pene erecto según las indicaciones del médico y las cuales el propio paciente debe tomarse desde su casa. Las erecciones espontáneas son casi siempre lo suficientemente buenas para fotografías debido a la dificultad que puede haber para que el paciente consiga una erección dentro del consultorio del médico.
La prueba de inyección intracavernosa puede producir erecciones de forma fisiológica e inducida pero debe evitarse en pacientes jóvenes con alto riesgo de priapismo. Se recomienda también, la medición de la longitud del pene cuando se realiza un abordaje quirúrgico y del cual se espera un acortamiento secundario (la técnica de rotación de los cuerpos tiene un mínimo riesgo de producir esto, véase más adelante).
No existe un método estándar de medición y la longitud del pene dependerá de la contracción de los músculos lisos del pene y de la grasa prepúbica, especialmente en pacientes con sobrepeso u obesos pero es importante realizar esta medición en diferentes momentos.
Sin embargo, la medición de ambos lados (corto y largo) de la longitud estirada es casi similar a la longitud eréctil, especialmente cuando la longitud estirada se tira tres veces antes de la medición. Esta simple prueba puede evitar las quejas de los pacientes y los padres, así como las reclamaciones legales.
¿Tiene solución la curvatura peneana?
La realidad es que sí. La curvatura congénita de pene es un problema que no tiene que ser para siempre en los hombres porque existen maneras de corregir el defecto.
Durante muchos años, la terapia de reemplazo de andrógenos se ha probado sin resultados consistentes en pacientes adultos. Por ende, la cirugía es la única opción de tratamiento para esta afección y se puede realizar en cualquier momento de la vida adulta. De hecho, un procedimiento quirúrgico de este tipo en edades tempranas podría evitar un impacto psicológico negativo.
Los tratamientos quirúrgicos para la curvatura congénita del pene generalmente comparten los mismos principios que la enfermedad de Peyronie, por ser trastornos similares. Es más, la mayoría de las técnicas utilizadas para la enfermedad de Peyronie (EP) se han descrito primero para la curvatura congénita del pene.
Tradicionalmente, las dos opciones quirúrgicas principales disponibles para el abordaje de la curvatura del pene incluyen:
- Acortar el lado más largo con escisiones o incisiones y plicatura.
- Alargamiento del lado más corto del pene erecto con injerto
Los pacientes con curvatura de pene, a diferencia de los pacientes con enfermedad de La Peyronie, generalmente tienen una buena longitud del pene y desafortunadamente, las técnicas quirúrgicas se centran principalmente en procedimientos que producen acortamiento como la plicatura o la incisión más plicatura.
Sin embargo, se han desarrollado algunas técnicas nuevas para reducir los efectos de acortamiento de las técnicas tradicionales con la misma corrección de la curvatura y la satisfacción del paciente y es acá donde hace su aparición, una nueva técnica: la técnica de rotación de cuerpos cavernosos de la que se hablará más adelante.
- VÍDEO: ¿Cómo eliminar la curva de pene sin perder tamaño?
Técnicas quirúrgicas para corregir la curvatura congénita de pene ¿Qué debo saber?
Las técnicas de reparación más utilizadas para las curvaturas simples del pene son el procedimiento Nesbit original, el procedimiento Nesbit modificado y la plicación. No obstante, en los últimos años se ha implementado un nuevo abordaje, con mejores resultados y menores complicaciones posteriores: la técnica de rotación de los cuerpos cavernosos.
Las plicaturas de la túnica albugínea en sus muchas variantes, han reportado muy buenos resultados en la corrección de la curvatura. En pacientes con curvatura severa del pene, la técnica de Nesbit proporciona resultados algo mejores que las técnicas de plicatura simple.
Se necesita un enfoque diferente para estos dos tipos principales de curvatura congénita del pene. Los principios generales de estas técnicas son similares a la enfermedad de Peyronie. Sin embargo, hay algunas peculiaridades que distinguen la curva congénita al abordar su tratamiento quirúrgico. Antes de la cirugía, es importante tener en cuenta las siguientes consideraciones:
- La juventud del paciente. Los pacientes generalmente se presentan después de alcanzar la pubertad a medida que la curvatura se vuelve más evidente. Muchos pacientes jóvenes se someten a cirugía antes de comenzar una relación sexual. Esto puede ser bastante beneficioso para evitar la ansiedad que existe al saber que el coito pueda ser doloroso o incómodo, no satisfactorio.
- Por lo general, no hay calcificación, ni induración de los cuerpos cavernosos, ni grosor asimétrico de la albugínea en ambos lados del pene (corto y largo). La presencia de nódulos fibrosos en el pene se refiere a la enfermedad de La Peyronie y por ello, el tratamiento es diferente aunque también, quirúrgico.
- La ausencia de placa retráctil calcificada en el lado más corto, la normalidad del tabique y la parte interna del cuerpo cavernoso y la ausencia de deformidades mayores son diferencias notables con respecto a la enfermedad de La Peyronie. Por lo general, hacen que el procedimiento sea más fácil.
- Se espera una curación normal después del procedimiento quirúrgico. No se han descrito trastornos de colágeno ni disfunción de curación en estos pacientes.
- El examen físico debe prestar especial atención al estado del cuerpo esponjoso, el meato urinario y la parte distal de la uretra. La conciencia del posible acortamiento uretral o la falta congénita de estas estructuras es el problema clínico más relevante a considerar en estos casos. Deben considerarse combinaciones de diferentes técnicas (uretroplastia con enderezamiento del pene) en el caso de trastornos uretrales.
Cirujanos que no tienen experiencia en este tipo de cirugías deben trabajar estrechamente con unidades especializadas en el tratamiento de la cirugía reconstructiva uretral, especialmente en los casos más severos de incurvación del pene. Estos casos deben ser manejados por un equipo multidisciplinario o cirujanos especialistas que tengan experiencia en el manejo de la uretra para evitar problemas.
¿En qué consiste la técnica de Nesbit?
Esta técnica consiste en acortar la túnica albugínea del lado contrario a la incurvación por medio de plicaturas (pequeños puntos de sutura) junto a cierta extracción de una porción de tejido e injerto en la túnica albugínea del lado afectado (o cóncavo). Con esto se consigue que la curvatura se disminuya y se rectifique.
Esta técnica ha representado el método quirúrgico más utilizado antes de la aparición de la técnica de rotación de cuerpos cavernosos, desarrollada por el Dr. Shaeer en 2006.
Esta cirugía comienza proporcionándole al paciente algo de anestesia local en el área genital, evitando así, la sedación nerviosa total. Esto es beneficioso a la hora de prevenir efectos adversos y reducir el tiempo de recuperación posterior a la anestesia.
Primero, se denuda al pene erecto por erección inducida haciendo una incisión anular en el prepucio, cerca de su unión con el glande. Así se consigue acceder a la túnica albugínea que, en el lado convexo, recibirá las plicaturas y a la que se le extraerá parte del tejido.
Una vez realizadas las plicaturas del tejido, se vuelve a unir el prepucio y la cirugía está completada.
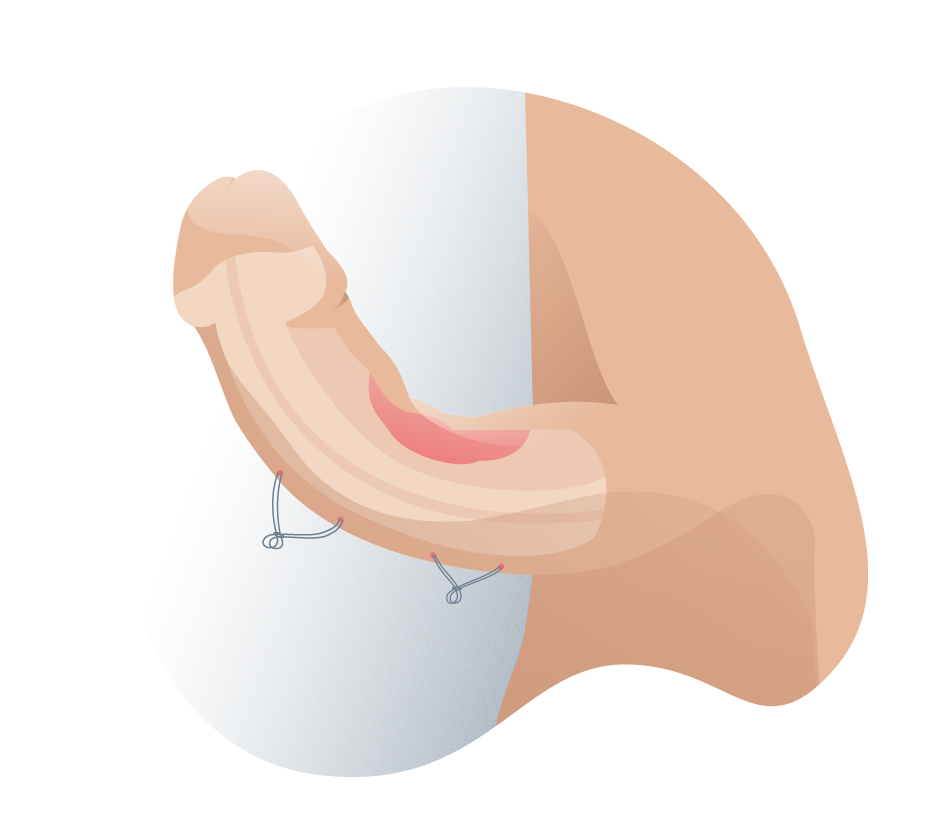
Aplicación de plicaturas mediante la técnica de Nesbit
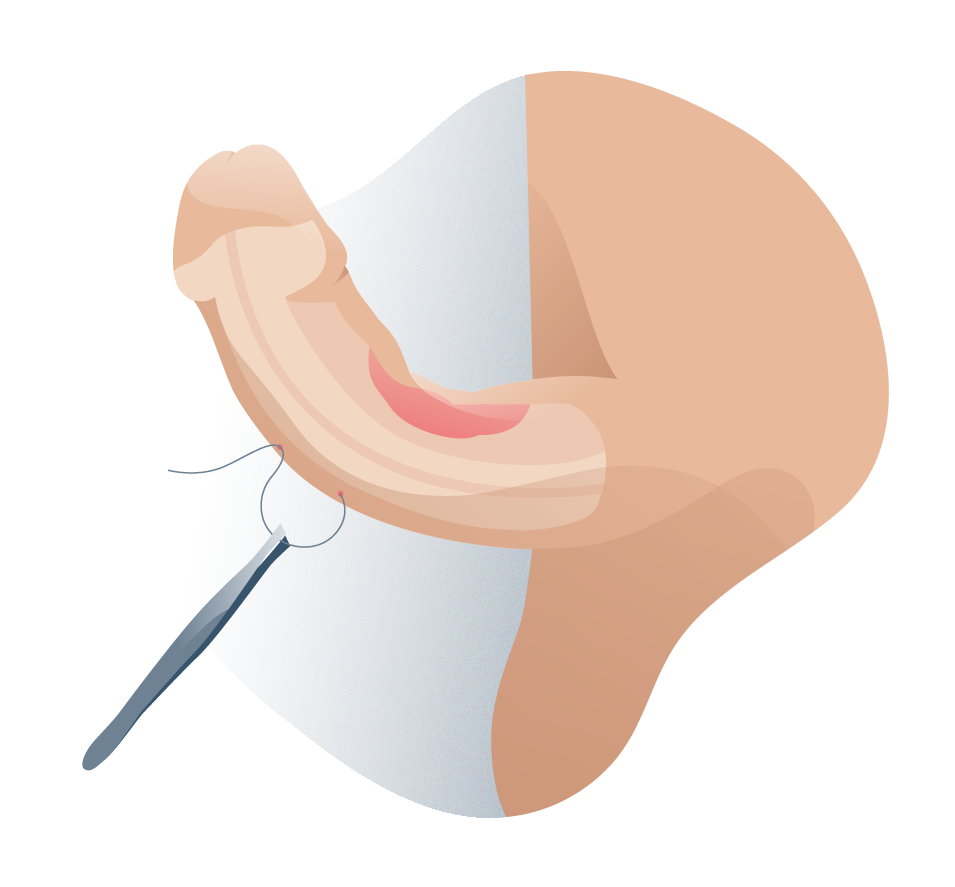
Corrección del pene mediante la técnica Nesbit
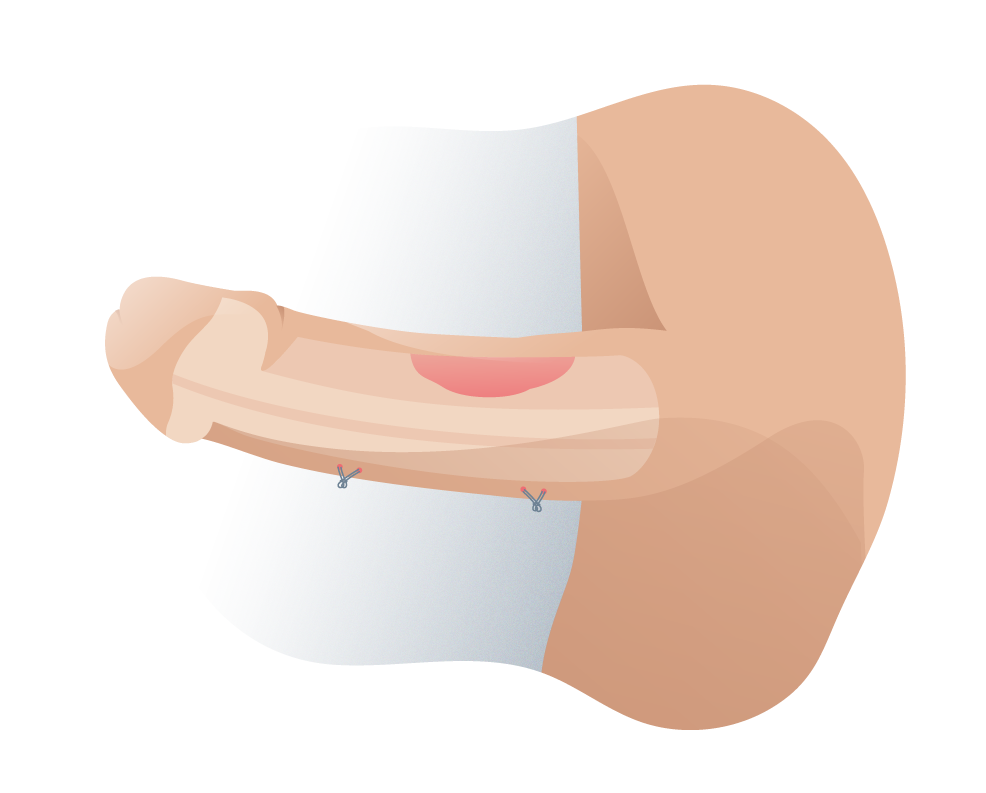
Técnica de Nesbit corregida
¿Qué es la técnica de rotación de cuerpos cavernosos de Shaeer y en qué consiste?
En 2006, el Dr. Shaeer publicó una nueva técnica desarrollada en El Cairo, basada en la rotación de los cuerpos cavernosos y actualizada por el mismo autor en 2008. Esta técnica innovadora reduce los efectos de acortamiento de las técnicas tradicionales con la misma corrección de la curvatura y con muy buenos resultados.
Esta técnica consiste en rotar lateralmente los cuerpos cavernosos de modo de que el pene adquiera un aspecto más recto. Esto se consigue accediendo a los cuerpos cavernosos por medio de una doble incisión en la parte dorsal o posterior del pene (una para cada cuerpo cavernoso) y realizando una doble sutura para forzarlos a mantener la rotación realizada.
La rotación de los cuerpos cavernosos, publicada por el Dr. Shaeer, es un tratamiento alternativo novedoso y útil que debe considerarse para los pacientes con curvatura congénita del pene, dada la facilidad de rendimiento y sus excelentes resultados.
Las nuevas modificaciones propuestas para la técnica han mejorado mucho más, sus resultados cosméticos y funcionales. Son particularmente útiles en casos de curvatura congénita severa del pene (cuando la incurvación supera los 60-90°).
Este procedimiento reduce el acortamiento del pene (riesgo que se corre con otras técnicas) y evita complicaciones como nódulos palpables, cicatrices en los cuerpos cavernosos y dolor en el pene.
A la técnica original se le han incorporado algunas modificaciones en la unidad de Andrología del hospital Virgen del Rocío de Sevilla (modificaciones lideradas por el Dr. Natalio Cruz de la Clínica Andromedi) y se realiza como se describe a continuación:
- Se denuda el pene a través de una incisión coronal y se realiza una erección artificial.
- Se diseca el paquete vasculonervioso en su totalidad y se realizan dos incisiones dorsales longitudinales en los cuerpos cavernosos, algo más separadas del septo y surco medio en la zona de máxima curva que en el resto.
- Luego se practica una doble sutura continua con monofilamento reabsorbible de larga duración 4/0: la primera une las caras internas y la segunda las externas. Esta doble sutura lograr cerrar ambos defectos a la par que imprime una rotación a los cuerpos cavernosos que endereza otras técnicas más propias del tratamiento de la estenosis de uretra o del hipospadias. La primera intervención quirúrgica, como en tantas situaciones de la medicina es la que ofrece las mayores oportunidades de curación al paciente. Por supuesto, el equipo quirúrgico debe dominar estas técnicas y estar preparado para solventar situaciones que de otro modo podrían ser perniciosas para la funcionalidad del pene.
- El acortamiento del pene que producen todas estas técnicas es algo que hay que dejar claro al indicar la intervención para evitar frustración en el paciente con el resultado quirúrgico. Este acortamiento supone uno de los mayores motivos de insatisfacción de los pacientes tras la cirugía. Por ello, algunas soluciones quirúrgicas empleadas en los últimos años como la de trasposición de albugínea en los centros de urología Andromedi de Madrid, Sevilla y Tenerife están dando resultados excelentes en términos de corrección de la curvatura congénita de pene con mínimo acortamiento de la longitud de éste.
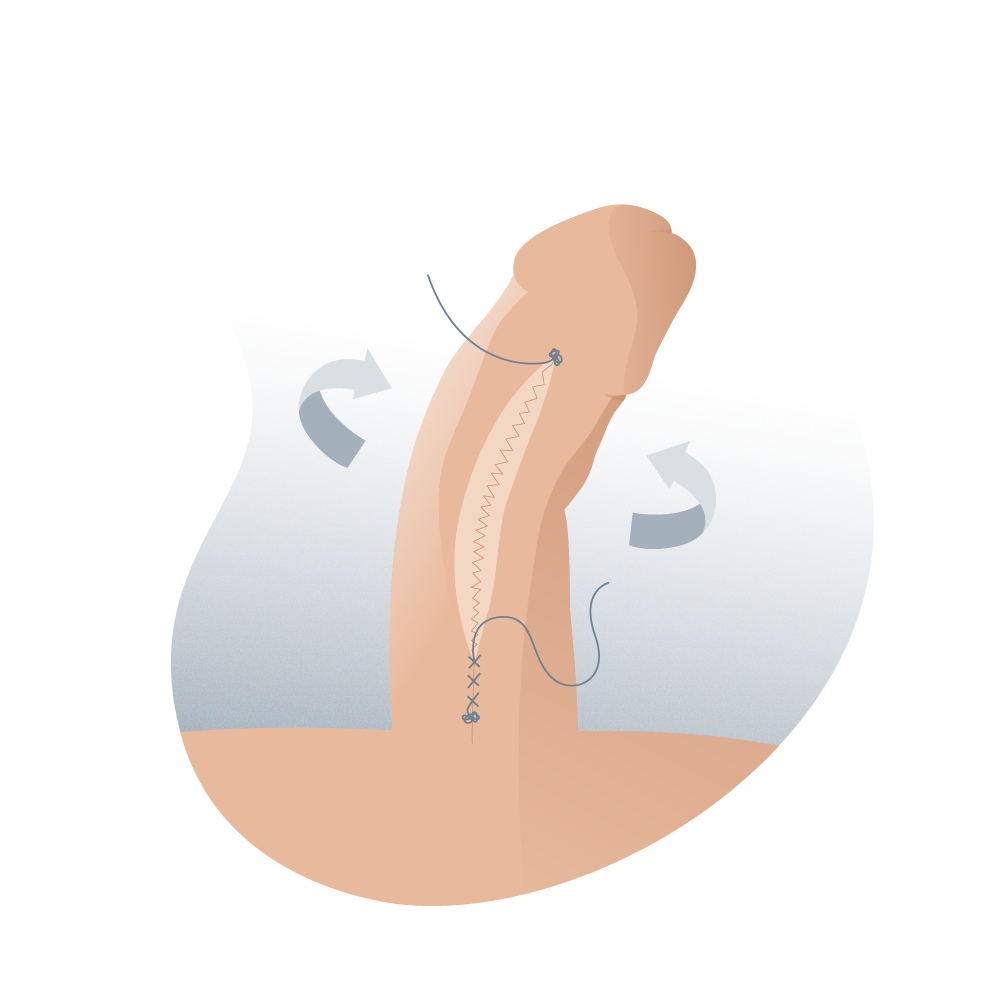
Técnica de rotación de cuerpos cavernosos
El paso a paso de la técnica de rotación de cuerpos cavernosos
Se realizó una incisión dorsal longitudinal en la parte dorsal de cada cuerpo cavernoso y, al suturar doblemente las partes internas y externas de la incisión se induce una rotación de los cuerpos cavernosos que produce un excelente enderezamiento del pene.
Paso 1
Después de administrar anestesia local en el pene (al igual que en todas las técnicas de corrección de curvatura peneana, congénita o adquirida) y de la desinfección del área a operar, el pene está listo para ser intervenido.
Paso 2
En la técnica original del Dr. Shaeer no se consideró necesaria la disección neurovascular. Sin embargo, este haz neurovascular (o paquete neurovascular) se puede diseccionar dorsalmente, especialmente si se necesita alguna plicatura o procedimiento adicional, evitando cualquier daño neurológico y vascular potencial.
Paso 3
Deben realizarse dos incisiones longitudinales superficiales en la parte dorsal de los cuerpos cavernosos, que involucran la capa longitudinal externa de la túnica albugínea, preservando la capa circular interna.
Estas dos incisiones deben ser ligeramente curvadas en lugar de paralelas, con una mayor separación en la parte central de la incisión. De hecho, cuanto más severa es la curvatura, mayor será la separación necesaria.
Paso 4
Primero, el cirujano realiza un cierre de los bordes interno o medial con una sutura continua. Luego, una segunda sutura continua se aproximará a los bordes laterales.
Lo ideal, de acuerdo a las recomendaciones del Dr. Shaeer, las sutura de poliglactina 910 (Vicryl), la poliglecaprona 25 (Monocryl) y la polidioxanona (PDS) parecen tener un perfil de retención de resistencia a la rotura muy largo y podrían ser una buena opción.
Paso 5
Acá, el cirujano induce una erección post quirúrgica y artificial para la medición del pene y así, poder evaluar la curvatura residual que pudiera quedar y los cambios que se pudieran hacer. El acortamiento de la longitud del pene suele ser bastante pequeño.
Paso 6
Se realiza el cierre de la fascia y piel de Buck con suturas de rápida absorción, catéter uretral y un apósito de compresión.
Preguntas frecuentes acerca de la técnica de rotación de cuerpos cavernosos mejorada por el Dr. Natalio Cruz.
Se han publicado muy buenos resultados con esta técnica como que:
• Se observó más del 90% de enderezamiento del pene en todos los casos.
• Con un acortamiento mínimo del pene (menor a un centímetro).
• Alta satisfacción del paciente en la recuperación de su vida sexual.
• Sin complicaciones postoperatorias.
Dentro de sus ventajas se encuentran:
• No deja cicatrices. La técnica de rotación de cuerpos cavernosos no produce cicatrices ni deja marcas que podrían arruinar el aspecto del pene debido al cuidadoso abordaje quirúrgico y el delicado proceso de cerrar el tejido abierto, son suturas delgadas.
• No deja nódulos en la parte dorsal del pene, como sí sucede con otras técnicas. Los nódulos aparecen cuando el tejido es unido nuevamente de una manera poco apropiada y ocurre un proceso de cicatrización exagerado, dando como resultado, acúmulos de tejido palpable debajo de la piel.
• Es anatómica y suave la corrección de la curvatura. Con la técnica de rotación de cuerpos cavernosos, el pene puede volver a tener erecciones uniformes y el paciente no suele percibir tensiones exageradas o incómodas. A simple vista, un pene que ha sido sometido a esta cirugía no se distingue de uno que nunca ha sido intervenido.
• No hay acortamiento del pene. Esta característica es por mucho, una de las más importantes de esta técnica. El pene puede alcanzar erecciones con la misma longitud que antes de la cirugía, no con menos. Esto se debe a que en ningún momento, rotar los cuerpos cavernosos implica acortar o reducir el tejido cavernoso del área incurvada.
Los pasos para recibir esta intervención quirúrgica constan de:
1. Exploración en consulta con fotografías del pene erecto para que el médico pueda examinar cuán grande es la curvatura anómala del pene y así poder evaluar las acciones a tomar para corregirla.
2. Se aplica anestesia local en la intervención quirúrgica, esto asegura que el procedimiento sea completamente indoloro.
3. La operación se realiza y el paciente puede regresar a casa.
El procedimiento en cuestión suele durar entre 4 y 16 horas en total, desde que el paciente llega al hospital hasta que sale de él. Todo dependerá de las necesidades del paciente y del tiempo que requiera para sentirse lo suficientemente bien para regresar a casa.
No es necesario que el paciente se quede en el hospital pero sí que tenga ciertos cuidados con la herida operatoria durante algunos días.
Lo ideal es que el paciente deba esperar algunos días para volver a retomar su vida sexual. Esto es con el fin de prevenir lesiones en el área recién operada. Las erecciones sostenidas, el coito o la masturbación podrían ser algo dolorosas durante un par de días después de la intervención.
Por mucho, la principal desventaja de la técnica convencional para reducir la curvatura congénita del pene, la técnica de Nesbit, es que produce un acortamiento en la longitud del pene erecto y que en muchos casos, puede ser mayor a un centímetro.
Esta característica puede hacer que muchos pacientes sientan temor de someterse a la operación. No obstante, con la técnica de rotación de cuerpos cavernosos, la disminución del tamaño del pene suele ser bastante pequeña y casi siempre, imperceptible.
Referencias médicas y bibliografía
- Penile Curvature (en inglés) European Association of Urology
- EAU – GUIDELINES ON PENILE CURVATURE (en inglés) European Association of Urology
- TRATADO DE ANDROLOGÍA - DR. NATALIO CRUZ 2DA. EDICIÓN, ESPAÑA - 2011
- H. PORST, Y. REISMAN. THE ESSM SYLLABUS OF SEXUAL MEDICINE EUROPEAN SOCIETY FOR SEXUAL MEDICINE. 2012. PAGES 927 – 951
BLOG ANDROMEDI
Otros artículos que te pueden interesar

Laparoscopic surgery for prostate
26 September 2023


Laser prostate surgery
22 November 2021


Impotence, incontinence and other problems after prostate surgery
22 November 2021
Author
Natalio Cruz MD, with 25 years of medical experience, has been until 2016 Head of the Andrology Unit in the Urology Service of the Virgen del Rocío Hospital in Seville, National Coordinator of Andrology in the Spanish Association of Urology (AEU) and General Secretary in the ESSM, positions that he has narrowed to focus squarely on this exciting project of offering a high-level private medical consultation in Marbella, Seville, Madrid and Tenerife.